🦷 Managing Bleeding in Dentistry — Translating Hemostasis, Pharmacology, and Risk into Clinical Decisions
- ToothOps

- Jul 8
- 3 min read
How clinicians think, plan, and guide healing when bleeding risk is real
🧠 Start Here: Why This Actually Matters
Every dental procedure is a controlled vascular injury.
In most cases:
the body responds predictably
a stable clot forms
healing proceeds
But when that system is altered—even slightly:
bleeding becomes prolonged
clot stability fails
healing becomes unpredictable
🧠 The Real Clinical Question
The question is not:
“Will this patient bleed?”
The real question is:
“Which component of hemostasis is most vulnerable under procedural stress—and how will that affect clot formation, stability, and resolution?”
🔥 ToothOps Insight
Bleeding is not failure—it is a readout of system behavior under stress.
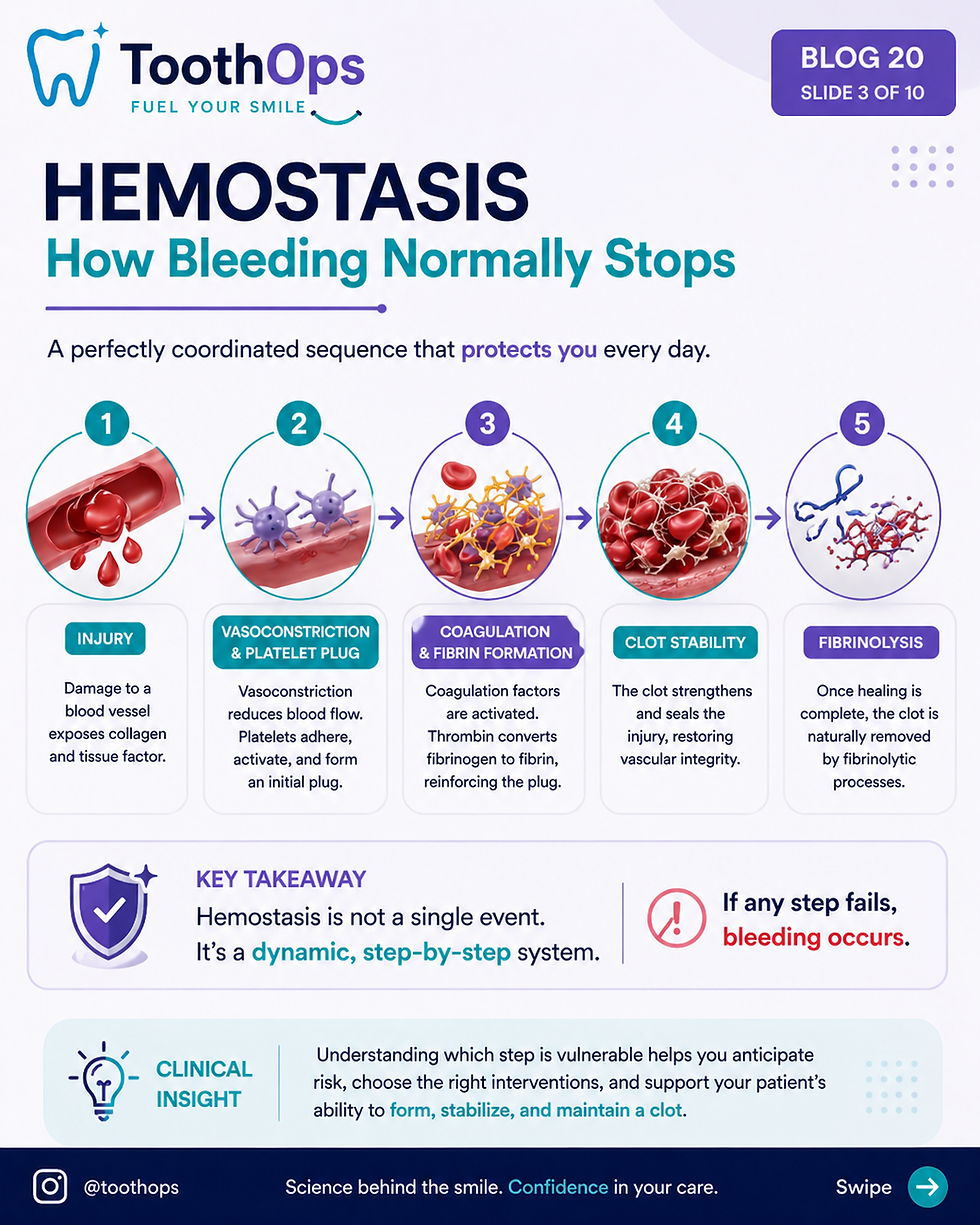
⚙️ Hemostasis in Dentistry: A System Under Load
Hemostasis is not linear—it is interdependent and dynamic.
🔬 The 4 Integrated Phases
Phase | Mechanism | Failure Pattern |
Vasoconstriction | transient vascular control | excessive initial bleeding |
Primary hemostasis | platelet adhesion (vWF), aggregation | immediate bleeding |
Secondary hemostasis | thrombin → fibrin | delayed bleeding |
Stabilization / fibrinolysis | clot reinforcement vs breakdown | re-bleeding |
🧠 Critical Insight
A clot must not only form—it must withstand mechanical and biochemical stress within the oral environment

🧠 ToothOps Clinical Model (HIGH-YIELD)
Bleeding can always be reduced to:
1. Formation
Can a clot form efficiently?
2. Amplification
Can thrombin generation reach a functional threshold?
3. Stability
Can the clot resist breakdown long enough for healing?
👉 This replaces memorization with functional reasoning
⚙️ Pre-Operative Risk Analysis (Where Outcomes Are Determined)
🔬 1. Hematologic Factors
platelet count AND function
coagulation factor integrity
thrombin generation capacity
🔬 2. Pharmacologic Modifiers
Drug Class | Mechanism | Clinical Effect |
Warfarin | ↓ II, VII, IX, X | delayed clot formation |
Heparin | ↑ antithrombin activity | prolonged coagulation |
DOACs | Xa or IIa inhibition | reduced thrombin generation |
Aspirin | COX inhibition | impaired platelet aggregation |
🧠 Advanced Insight
Factor Xa inhibitors reduce thrombin generationDirect thrombin inhibitors reduce thrombin activity
🔬 3. Tissue-Level Biology
From gingival vascular structure:
dense capillary plexus
high perfusion
rapid inflammatory response
🧠 Clinical Insight
Inflammation shifts the local environment from anti-thrombotic → pro-bleeding through vascular fragility
⚙️ Intraoperative Hemostasis: Mechanism-Based Control
🧩 Local Control Strategies
Method | Mechanism |
Pressure | promotes platelet adhesion |
Sutures | reduce shear + stabilize clot |
Collagen/Gelfoam | scaffold for fibrin |
Epinephrine | reduces perfusion |
🧠 High-Level Insight
Local hemostasis does not replace systemic clotting—it compensates for its limitations
⚠️ Clot Stability: The Most Underestimated Variable
🔬 The Problem
Even with normal clot formation:
👉 fibrinolysis may dominate
🔬 Mechanism
plasmin degrades fibrin
oral cavity = high fibrinolytic activity
💊 Intervention
Drug | Mechanism |
Tranexamic acid | inhibits plasminogen activation |
EACA | stabilizes fibrin matrix |
🧠 Critical Insight
Hemostasis is not binary (clot vs no clot)👉 it is a balance between formation and dissolution

🦷 Real Clinical Scenario (HIGH-YIELD)
A patient returns 6–12 hours post-extraction with bleeding.
Mechanistic Interpretation:
initial clot formed
thrombin generation adequate
fibrinolysis exceeded stability
Diagnosis:
👉 Clot instability—not clotting failure
Management:
re-establish clot
reduce mechanical disruption
consider antifibrinolytics
🧠 ToothOps Insight
Delayed bleeding is rarely about starting the clot
👉 it is about maintaining it

⚙️ Post-Operative Phase: Environmental Stress
Key Stressors:
saliva enzymes
mechanical movement
negative pressure
🧠 Clinical Translation
The oral cavity is one of the most hostile environments for clot stability
⚠️ High-Risk Profiles
🔴 Anticoagulated Patients
→ impaired thrombin generation
🔴 Liver Disease
→ reduced factor synthesis
🔴 Thrombocytopenia
→ weak primary plug
🔴 DIC / systemic disorders
→ simultaneous clotting and depletion

🧠 Integrated Clinical Framework
Question | Interpretation |
Timing | platelet vs factor |
Location | surface vs deep |
Pattern | formation vs breakdown |
Context | systemic vs local |
🧠 Final ToothOps Insight
Bleeding is not unpredictable—it is patterned system behavior

✨ Final Takeaway
Bleeding in dentistry is not a complication to fear.
It is a system to understand.
The difference between routine healing and complicationis not technique alone—
it is the clinician’s ability to interpret and guide biology.
🧠 Why This Matters
Because every procedure:
challenges hemostasis
tests clot stability
depends on your ability to anticipate failure
When you understand the system,you stop reacting—
and start making decisions that prevent problems before they begin.
@ToothOps | Fuel Your Smile 😊
Stay tuned for more insights and educational content in our blog.
Disclaimer: Content is for educational purposes only and not a substitute for medical or dental care.
© 2025 ToothOps | All Rights Reserved.


Comments