🦷 Why a Tiny Blockage Can Shut Down Your Entire System
- ToothOps

- 1 day ago
- 7 min read
The Hidden Flow System Behind Bile, Digestion,
Think like a clinician. Understand like a patient. Remember like a visual system.

BIG PICTURE: The Body Is a Flow System
Most people think disease starts when something is “damaged.”
But many serious conditions begin when something is blocked.
A tiny obstruction can stop the movement of:
Flow Type | What Moves | Why It Matters |
Bile flow | bile from liver/gallbladder → intestine | digests fat, carries bilirubin/waste |
Pancreatic flow | enzymes from pancreas → intestine | digests proteins, fats, carbs |
Portal venous flow | nutrient-rich blood from gut/spleen/pancreas → liver | detoxification, metabolism, nutrient processing |
Mental model:The liver is both a filter and a factory.
Filter: portal vein brings blood from the gut, spleen, pancreas, and intestines to the liver.
Factory: liver makes bile and sends it out through ducts.
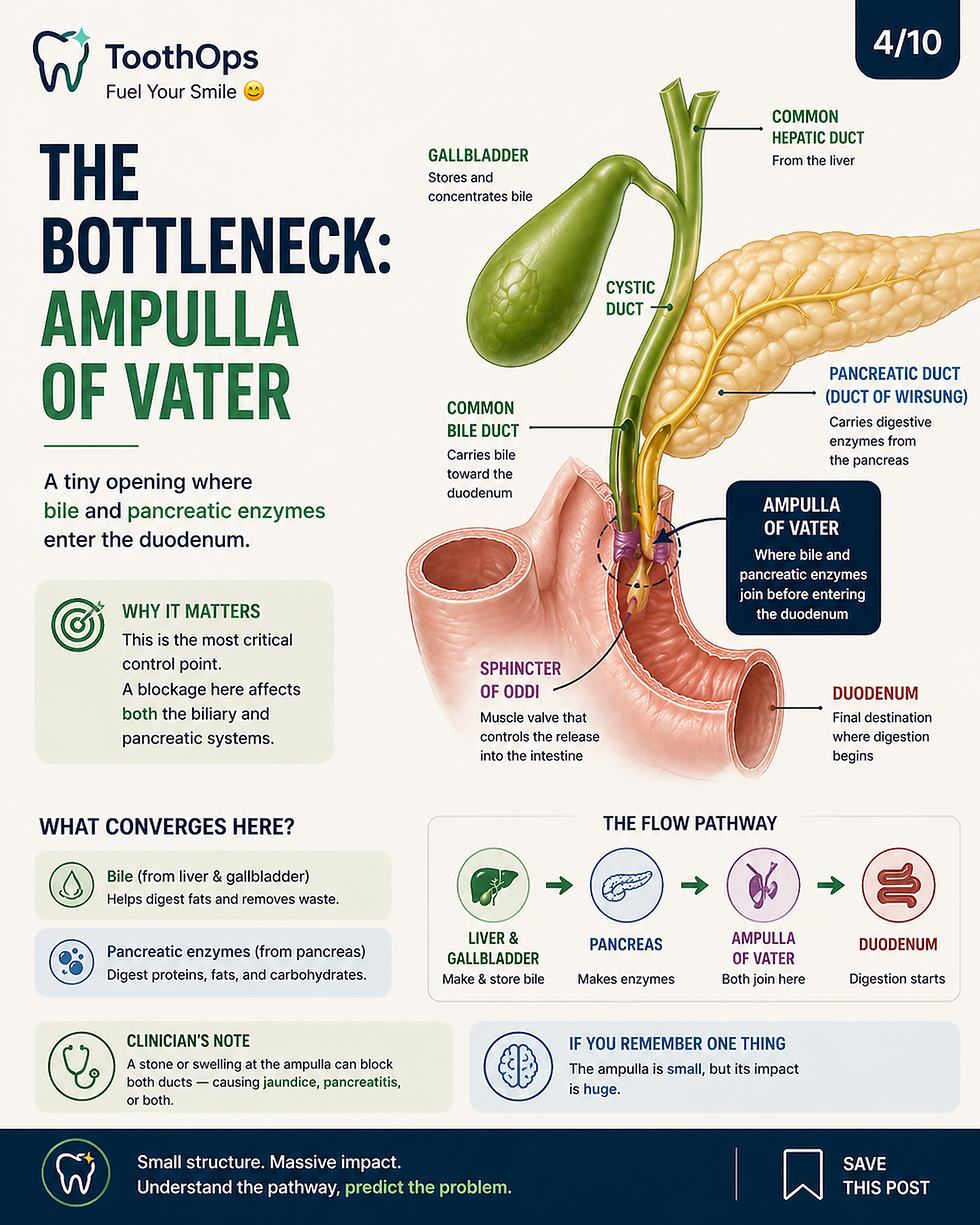
Bottleneck: bile and pancreatic enzymes meet near the ampulla of Vater before entering the duodenum.

1. The Route of Bile: The Excretion Pathway
Bile is produced by hepatocytes, then travels through increasingly larger ducts until it reaches the intestine.
Bile Flow Route
Step | Structure | Function |
1 | Hepatocytes | produce bile |
2 | Bile canaliculi | microscopic channels between hepatocytes |
3 | Intrahepatic ducts | collect bile inside liver |
4 | Right + left hepatic ducts | drain right and left liver lobes |
5 | Common hepatic duct | main liver drainage duct |
6 | Cystic duct | connects gallbladder |
7 | Common bile duct | carries bile toward duodenum |
8 | Ampulla of Vater | common channel with pancreatic duct |
9 | Sphincter of Oddi | controls entry into duodenum |
10 | Duodenum | bile enters digestion |
The common bile duct and pancreatic duct unite near the ampulla of Vater, and the sphincter of Oddi regulates flow into the duodenum.
If you only remember one thing:
Bile is made in the liver, stored in the gallbladder, and released into the duodenum through a shared exit point with the pancreas.
2. The Route of Pancreatic Enzymes: The Digestive Enzyme Pathway
The pancreas releases enzymes that digest food.
Pancreatic Flow Route
Structure | Role |
Acinar cells | produce digestive enzymes |
Small pancreatic ducts | collect enzyme-rich fluid |
Duct of Wirsung | main pancreatic duct |
Ampulla of Vater | joins bile duct outflow |
Sphincter of Oddi | controls release into duodenum |
Duodenum | enzymes digest food |
The duct of Wirsung is the main pancreatic duct and carries pancreatic secretions toward the ampulla of Vater.
Why this matters:
Pancreatic enzymes are powerful. They are supposed to activate in the intestine — not inside the pancreas.
If blocked, enzyme flow can back up, contributing to acute pancreatitis.
3. The Route of Portal Blood: The Input Pathway
The liver does not only send bile out. It also receives blood in.
Most nutrient-rich venous blood from the digestive system travels to the liver first through the portal venous system.
Portal Venous Route
Route | Meaning |
Gut absorbs nutrients/toxins | digestion products enter venous blood |
SMV drains much of intestine | superior mesenteric vein |
Splenic vein drains spleen, pancreas, stomach region | important portal tributary |
SMV + splenic vein → portal vein | major portal vein formation |
Portal vein enters liver | blood is processed |
Sinusoids → central veins | liver microcirculation |
Hepatic veins → IVC | blood returns to systemic circulation |
The superior mesenteric vein joins the splenic vein behind the neck of the pancreas to form the portal vein.
If you only remember one thing:
SMV + splenic vein = portal vein → liver.

4. The Core Anatomical Bottleneck: Ampulla of Vater
The ampulla of Vater is a small but high-impact junction where bile and pancreatic secretions enter the duodenum.
Why It Is Clinically Powerful
If the blockage is here… | What happens |
Bile cannot drain | bilirubin backs up → jaundice |
Pancreatic enzymes cannot drain | enzyme trapping → pancreatitis risk |
Duct pressure rises | pain, inflammation, duct dilation |
Bacteria ascend | cholangitis risk |
Infection enters blood | sepsis risk |
Stones obstructing the ampulla of Vater can cause gallstone pancreatitis, and more complete bile duct obstruction can lead to jaundice and ascending cholangitis.
5. Mechanism: How a Small Stone Causes Big Disease
Step-by-Step Pathway
Step | Mechanism | Clinical Result |
1 | Gallstone blocks duct | interrupted flow |
2 | Bile cannot exit | duct pressure rises |
3 | Bilirubin accumulates | jaundice, dark urine, pale stools |
4 | Bile stagnates | bacterial overgrowth risk |
5 | Pancreatic outflow blocked | enzyme trapping |
6 | Inflammation amplifies | pancreatitis/cholangitis |
7 | Bacteria/toxins enter blood | sepsis risk |
Biliary obstruction means impaired bile flow from the liver into the intestinal tract.

6. Clinical Pattern Recognition: Location Predicts Disease
Obstruction Location Table
Blockage Location | Main Disease Pattern | Key Clues |
Cystic duct | Cholecystitis | RUQ pain, fever, gallbladder inflammation |
Common bile duct | Choledocholithiasis / obstructive jaundice | jaundice, dark urine, pale stool, ↑ bilirubin/ALP |
Ampulla of Vater | Gallstone pancreatitis + jaundice | epigastric pain radiating to back, ↑ lipase |
Intrahepatic ducts | Intrahepatic cholestasis | cholestatic labs, itching |
Post-surgical accessory duct injury | bile leak | pain, biloma, postoperative leak |
ToothOps Insight:
Anatomy is prediction. Where the blockage sits tells you what system fails next.
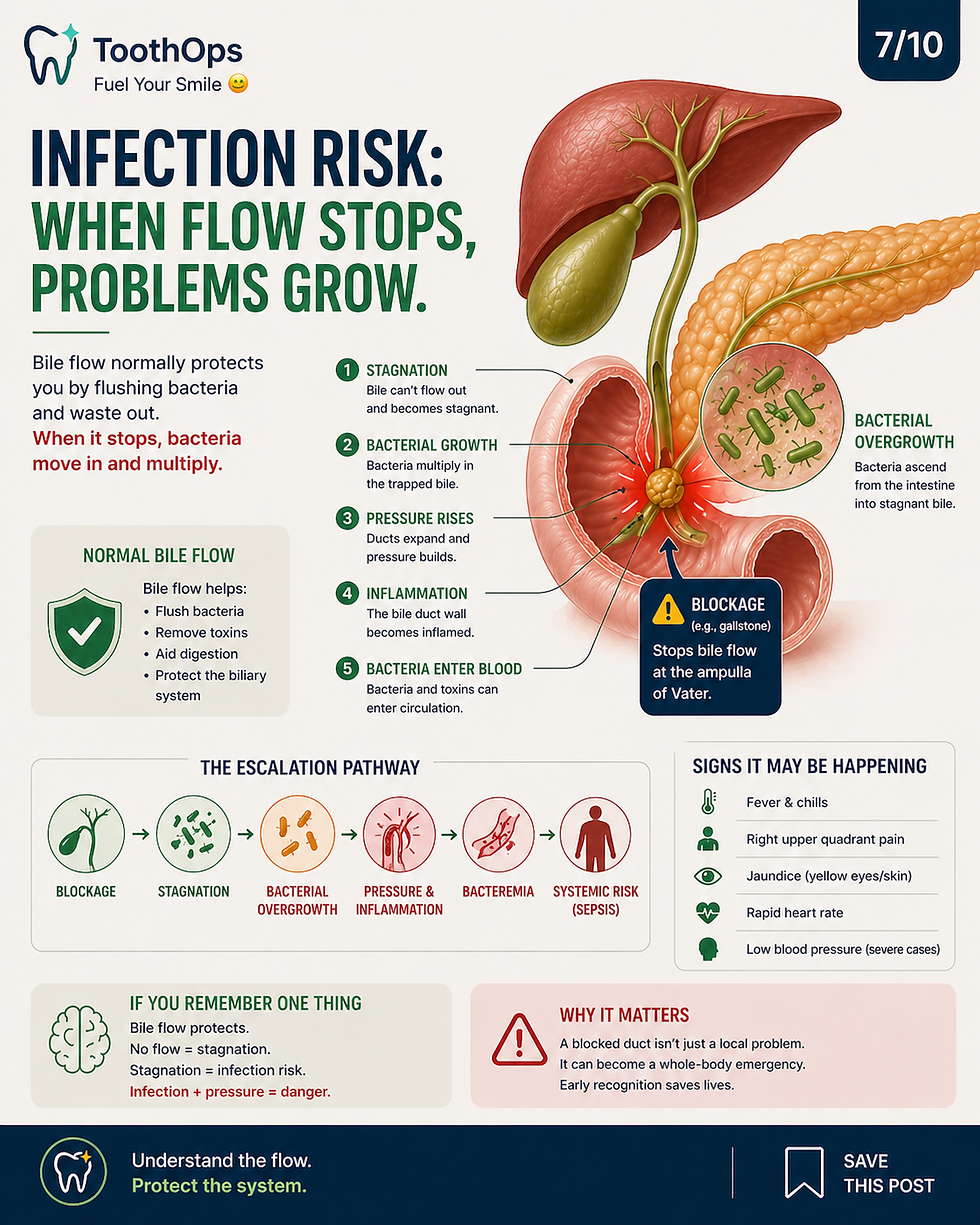
7. Why Sepsis Belongs in This Blog
Sepsis should not be added randomly.
It belongs as the final escalation of obstruction + infection + systemic spread.
Normal Flow Protects You
Bile flow normally helps prevent stagnation and bacterial buildup.
When bile stops moving:
Bile stagnates
Bacteria ascend from the intestine
Duct pressure rises
Bacteria and inflammatory toxins enter circulation
The immune system becomes systemically activated
Blood pressure can fall
Organs can become underperfused
This is how a duct problem can become a whole-body emergency.
Acute cholangitis is inflammation of the bile ducts, often caused by infection or blockage such as a gallstone, and is considered an emergency.
8. Ascending Cholangitis: The Infection Pattern
Classic Pattern
Syndrome | Findings |
Charcot’s triad | fever + jaundice + right upper quadrant pain |
Reynolds pentad | Charcot’s triad + hypotension + altered mental status |
Reynolds pentad reflects severe disease with systemic instability.
Patient-friendly explanation:
A blocked bile duct can trap infected fluid under pressure. If bacteria enter the bloodstream, the body may respond with widespread inflammation, low blood pressure, confusion, and organ stress.
9. Lab Interpretation Framework
Biliary vs Pancreatic Pattern
Lab | Why It Changes | Pattern |
Total/direct bilirubin | bile pigment cannot drain | ↑ in obstruction |
ALP | bile duct epithelial stress | ↑ cholestatic pattern |
GGT | biliary tract/liver enzyme | supports hepatobiliary source |
AST/ALT | hepatocyte injury or pressure-related injury | variable ↑ |
Lipase | pancreatic injury/enzyme leakage | ↑ pancreatitis |
WBC | infection/inflammation | ↑ cholangitis/sepsis |
Lactate | tissue hypoperfusion | ↑ severe sepsis/shock |
Clinical logic:
High bilirubin + high ALP/GGT → think bile flow problem
High lipase + epigastric pain → think pancreatic involvement
Fever + hypotension + confusion → think systemic infection/sepsis risk
10. Micro-Level Liver Physiology: Blood and Bile Move Opposite Directions
Inside the liver lobule:
Flow | Direction |
Blood | portal triad → sinusoids → central vein |
Bile | hepatocytes → canaliculi → bile ducts |
This means the liver is organized like a counter-flow processing system.
Why It Matters
Mechanism | Result |
Bile obstruction | bile acids and bilirubin accumulate |
Increased duct pressure | hepatocyte stress/injury |
Reduced oxygen delivery | vulnerable zones suffer injury |
Inflammation | worsens duct and liver damage |
If you only remember one thing:
Blood flows in for processing. Bile flows out for excretion. Disease happens when that traffic pattern breaks.
11. Important Named Structures
High-Yield Anatomy Table
Structure | What It Is | Why It Matters |
Splenic vein | drains spleen and contributes to portal vein | joins SMV to form portal vein |
Portal vein | carries gut/spleen/pancreas blood to liver | liver detoxification/metabolism |
Duct of Wirsung | main pancreatic duct | enzyme flow to duodenum |
Ampulla of Vater | shared exit of bile + pancreatic duct | obstruction can cause jaundice + pancreatitis |
Sphincter of Oddi | smooth muscle valve | regulates bile/pancreatic release |
Ducts of Luschka | accessory/subvesical bile ducts near gallbladder bed | injury can cause bile leak after cholecystectomy |
Ducts of Luschka are accessory bile ducts near the gallbladder bed and are clinically relevant because injury during cholecystectomy can cause bile leak.
12. Dentistry-Specific Relevance
This topic is not “just GI.”
It matters in dentistry because dental care often intersects with systemic disease.
Dental Implications
Situation | Why It Matters in Dentistry |
Jaundice/liver dysfunction | altered drug metabolism, bleeding risk |
Cholangitis/sepsis history | medical stability and timing of care matter |
Pancreatitis hospitalization | defer elective care during acute illness |
Liver disease/portal hypertension | thrombocytopenia, coagulopathy, infection risk |
Antibiotic use | medication history and hepatic dosing considerations |
Oral signs of systemic illness | pallor, jaundice, bleeding tendency may be visible |
Clinical dental reasoning:
Before elective procedures, ask:
Is the patient medically stable?
Are liver enzymes/bilirubin abnormal?
Are platelets or coagulation factors affected?
Is there active infection or fever?
Are medications hepatically metabolized?
Does the patient need medical clearance?
13. Clinical Reasoning Framework
The ToothOps 5-Step Flow Framework
Step | Question | Why It Matters |
1 | What flow is blocked? | bile, enzymes, blood |
2 | Where is the blockage? | cystic duct, CBD, ampulla |
3 | What backs up? | bilirubin, bile acids, enzymes |
4 | What becomes inflamed or infected? | gallbladder, bile ducts, pancreas |
5 | Has it become systemic? | fever, hypotension, confusion, sepsis |
14. Short Clinical Case Example
A patient presents with:
Right upper quadrant pain
Fever
Yellow eyes
Dark urine
Low blood pressure
Reasoning Walkthrough
Finding | Interpretation |
RUQ pain | biliary tract irritation |
Jaundice | impaired bile drainage |
Fever | infection/inflammation |
Dark urine | conjugated bilirubin entering urine |
Low blood pressure | systemic inflammatory response concern |
Clinical pattern:
This is not just “gallbladder pain.”
This suggests possible biliary obstruction with infection, and systemic instability raises concern for sepsis.
15. Common Misconceptions and Exam Traps
Misconception | Correction |
“Gallstones only affect the gallbladder.” | They can obstruct the common bile duct or ampulla. |
“Jaundice means liver failure.” | It can also mean bile cannot drain. |
“Pancreatitis is always alcohol-related.” | Gallstones are a major cause of acute pancreatitis. |
“Sepsis starts only from obvious infections.” | A blocked infected duct can cause sepsis. |
“Anatomy is memorization.” | Anatomy predicts symptoms, labs, and urgency. |
16. Chairside Explanation
“Your body has small pathways that move bile and digestive enzymes into the intestine. If one of those pathways gets blocked, pressure can build up behind it. That can cause pain, yellowing of the eyes, inflammation of the pancreas, or even infection. The reason clinicians take this seriously is because a small blockage can affect multiple organs and, in severe cases, spread infection into the bloodstream.”

ToothOps Insight
Small anatomy can create massive consequences when it controls flow.
The body does not only break from damage.It can break from interruption.
Final Takeaway
If you understand the route, you can predict the disease.
Block bile → jaundice
Block enzymes → pancreatitis
Block infected bile → cholangitis
Let infection spread → sepsis
That is why anatomy is not memorization.
It is clinical prediction.
@ToothOps | Fuel Your Smile 😊
Stay tuned for more insights and educational content in our blog.
Disclaimer: Content is for educational purposes only and not a substitute for medical or dental care.
© 2025 ToothOps | All Rights Reserved.



Comments