🦷Why the Body Turns Yellow
- ToothOps

- 3 days ago
- 6 min read
A Systems-Level Guide to Bilirubin Flow, Liver Function, and Hidden Disease

Big Picture: Jaundice Is a Flow Problem
Jaundice is not a disease by itself.
It is a visible sign that the body’s bilirubin system is not keeping up.
Think of bilirubin like waste from old red blood cells. The body must:
Step | Job | Main Organ/System |
1. Produce | Break down old red blood cells | Spleen, macrophages |
2. Process | Convert bilirubin into a removable form | Liver |
3. Move | Send bilirubin through bile into the intestine | Bile ducts |
4. Eliminate | Remove it through stool and urine pathways | Intestine, kidney |
The simple model:
Too much produced, not enough processed, or blocked from leaving → bilirubin builds up → yellow color appears.

1. Where Bilirubin Comes From
Bilirubin begins with red blood cell turnover.
Old red blood cells are broken down mainly by macrophages in the spleen, liver, and bone marrow. Hemoglobin is separated into globin and heme. Heme is converted into biliverdin, then into unconjugated bilirubin.
If you only remember one thing
Bilirubin is the body’s waste product from heme breakdown.
The First Key Distinction: Unconjugated vs Conjugated
Type | Meaning | Solubility | Main Problem If Elevated |
Unconjugated bilirubin | Not yet processed by liver | Fat-soluble | Too much production or poor liver uptake/conjugation |
Conjugated bilirubin | Processed by liver | Water-soluble | Poor bile flow or impaired secretion |
This distinction matters because it tells the clinician where the problem likely is.
2. The Liver as a Biochemical Transformer
The liver does not simply “filter” bilirubin.
It transforms bilirubin.
Unconjugated bilirubin travels to hepatocytes, where it is conjugated with glucuronic acid. This makes bilirubin water-soluble enough to be secreted into bile.
Big Picture
Before Liver Processing | After Liver Processing |
Unconjugated bilirubin | Conjugated bilirubin |
Fat-soluble | Water-soluble |
Harder to excrete | Ready for bile elimination |
The liver is therefore a chemical processing center. When hepatocytes are injured, inflamed, infected, or overwhelmed, bilirubin handling becomes abnormal.
This connects directly to viral hepatitis B/C and immune-mediated liver injury, both listed in your case study guide.
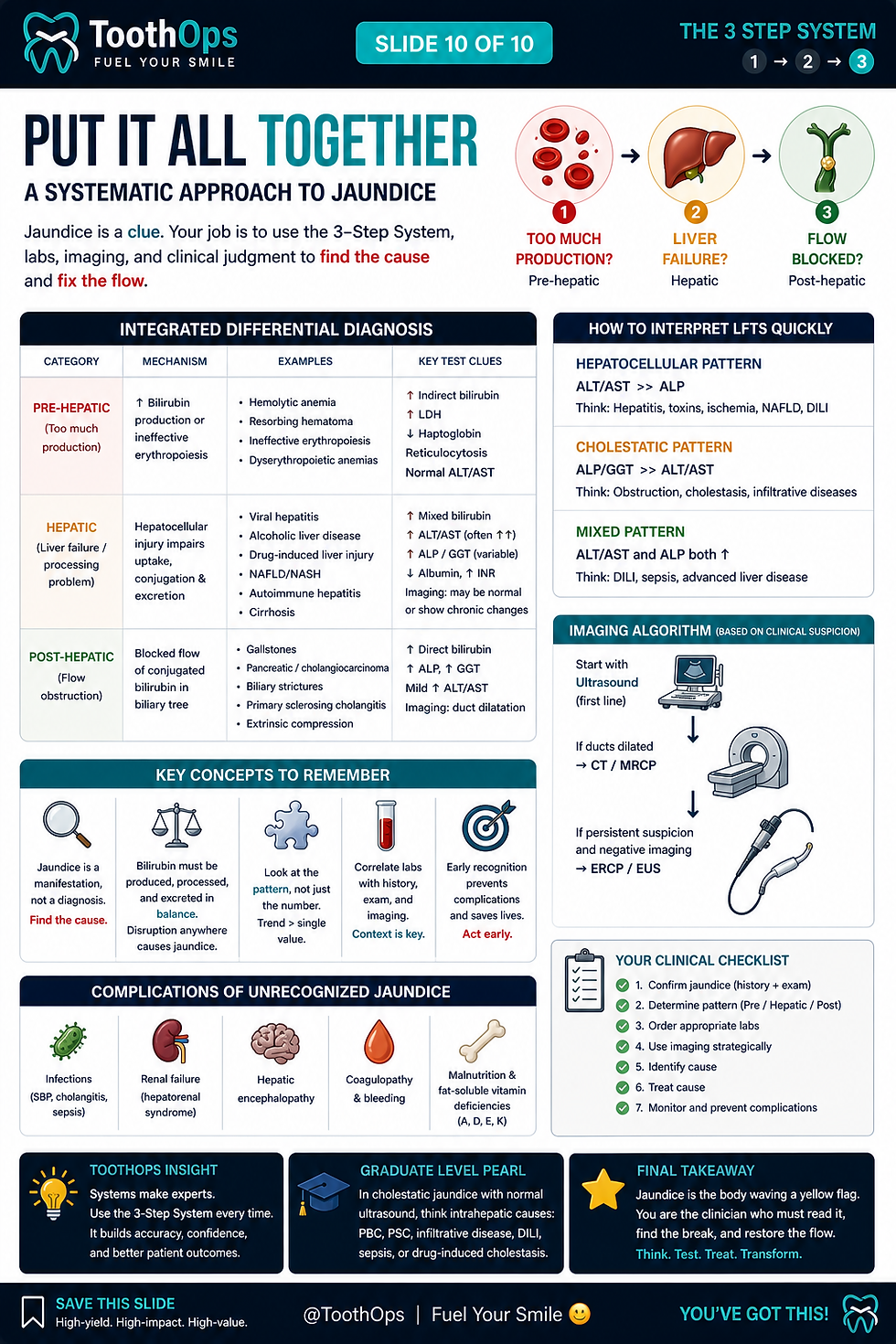
3. The Three Major Patterns of Jaundice
Clinicians do not just ask, “Is the patient yellow?”
They ask:
Where is bilirubin flow breaking down?
Master Framework
Type of Jaundice | Problem Location | Main Mechanism | Big Clue |
Pre-hepatic | Before liver | Too much RBC breakdown | Unconjugated bilirubin rises |
Hepatic | Inside liver | Hepatocyte processing/secretion problem | Mixed liver dysfunction picture |
Post-hepatic | After liver | Bile cannot flow out | Conjugated bilirubin backs up |
1. Pre-Hepatic Jaundice: Too Much Input
This happens when red blood cells are breaking down faster than the liver can process the bilirubin load.
Examples:
hemolysis
transfusion reaction
increased RBC destruction
The liver may be working normally, but the system is overloaded.
Production exceeds processing capacity.
2. Hepatic Jaundice: Processing Failure
This happens when hepatocytes cannot properly uptake, conjugate, or secrete bilirubin.
Examples:
viral hepatitis
cirrhosis
toxin or medication injury
immune-mediated liver damage
This is where hepatitis becomes clinically important. The virus itself may infect hepatocytes, but much of the liver injury can come from the immune response trying to control infected cells.
The processing center is damaged.
3. Post-Hepatic Jaundice: Flow Obstruction
This happens when conjugated bilirubin is made but cannot exit normally through bile.
Examples:
gallstones
tumors
strictures
fibrosis affecting flow
Because conjugated bilirubin is water-soluble, it can spill into blood and urine.
The exit pathway is blocked.
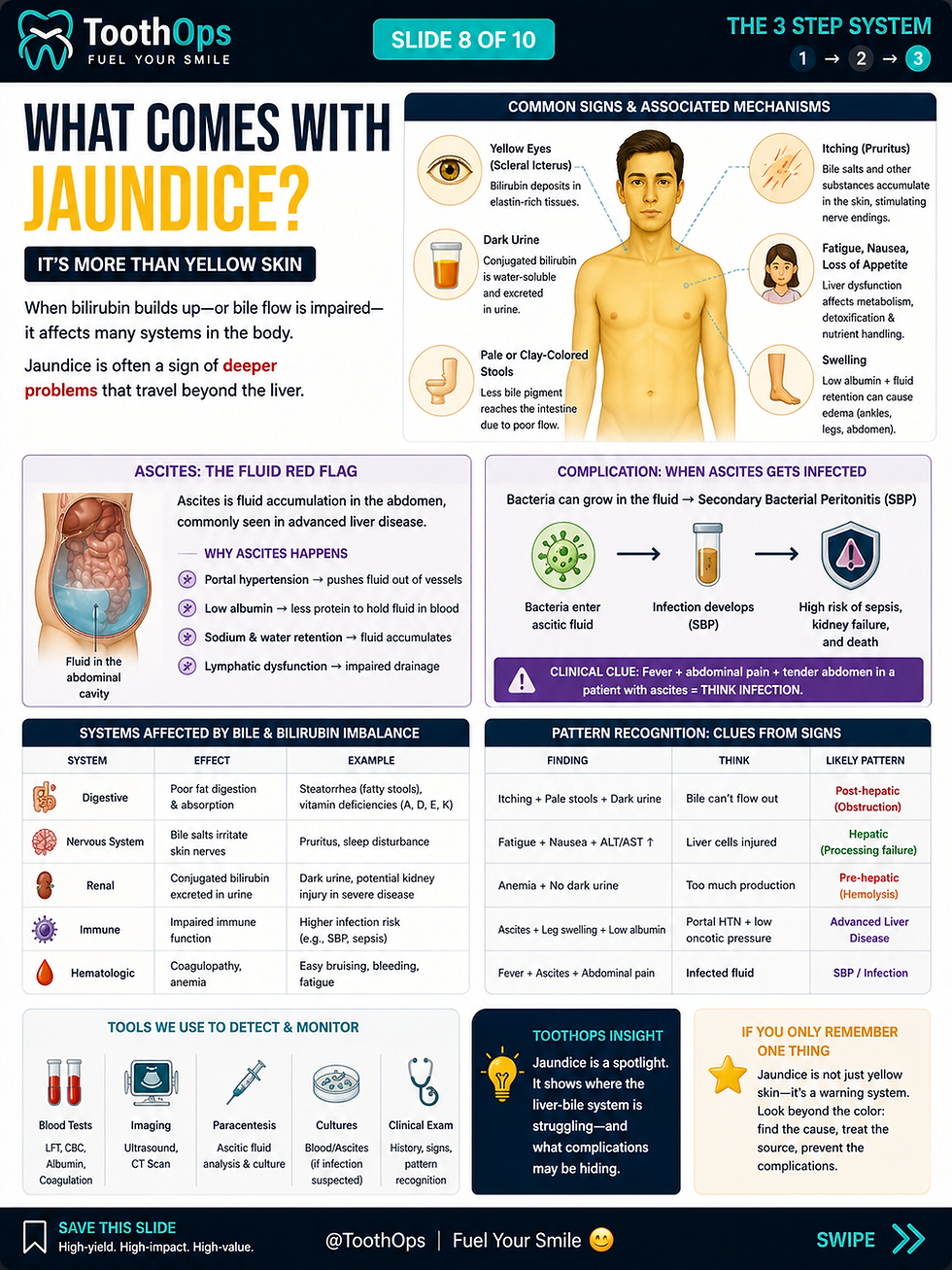
4. Why the Body Looks Yellow
Bilirubin accumulates in tissues.
The yellow color often appears in:
sclera of the eyes
skin
mucous membranes
The sclera often shows jaundice early because bilirubin has affinity for elastin-rich tissues.
ToothOps Insight
The eyes can become a visible window into liver, blood, and bile flow physiology.
5. Why Jaundice Often Comes With Itching
Itching is not random.
In cholestatic or obstructive patterns, bile-related compounds can accumulate and stimulate sensory nerves in the skin. Your study guide specifically lists “itching mechanism” as part of this case system, which makes it important to connect jaundice with nerve signaling, not just liver color changes.
Mechanism Model
Finding | Mechanism |
Yellow skin/eyes | bilirubin deposition |
Itching | bile-related mediators stimulate cutaneous nerves |
Dark urine | conjugated bilirubin reaches urine |
Pale stool | less bile pigment reaches intestine |

6. Why Ascites Can Appear With Liver Disease
Jaundice may occur with other signs of liver dysfunction, including ascites.
Ascites means fluid accumulation in the abdominal cavity. It is not simply “extra water.” It reflects disrupted pressure and protein balance.
Major contributors:
portal hypertension
reduced albumin production
sodium/water retention
systemic vascular changes
Your case guide links portal circulation, portal hypertension, ascites, blood/ascites cultures, and secondary bacterial peritonitis, which means ascites should be taught as part of a broader liver-system failure pattern.
Ascites Framework
Problem | Effect |
Portal hypertension | pushes fluid out of circulation |
Low albumin | reduces plasma oncotic pull |
Immune dysfunction | increases infection risk |
Fluid accumulation | creates space where bacteria can grow |
Clinical escalation
Ascites can become dangerous when infected, leading to secondary bacterial peritonitis or related intra-abdominal infection patterns. This is why fluid is not passive; it can become a biologically active risk environment.
7. Diagnostic Thinking: Labs Locate the Failure Point
Clinicians use labs not just to confirm jaundice, but to determine where the system is failing.
Your guide lists alanine aminotransferase, alpha-fetoprotein, PCR, branched-chain complementary DNA assay, liver biopsy, and cultures as relevant diagnostic topics.
High-Yield Diagnostic Table
Test | What It Helps Reveal |
Total bilirubin | overall bilirubin burden |
Direct bilirubin | conjugated bilirubin level |
Indirect bilirubin | unconjugated bilirubin estimate |
ALT | hepatocyte injury |
AST | hepatocyte or systemic tissue injury |
ALP/GGT | cholestasis or bile duct involvement |
PCR | viral genetic material |
AFP | liver cancer risk marker in certain contexts |
Liver biopsy | tissue-level diagnosis |
Blood/ascites cultures | infection source |
Pattern Recognition Table
Pattern | Think |
High indirect bilirubin | hemolysis or impaired conjugation |
High direct bilirubin | obstruction or impaired secretion |
High ALT/AST | hepatocyte injury |
High ALP/GGT | bile flow problem |
Fever + ascites | possible infected fluid |
8. Hepatitis Connection: Why Silent Disease Matters
Hepatitis B and C can damage the liver quietly over time.
The danger is that the patient may feel normal while inflammation, fibrosis, and impaired liver function develop slowly.
Big Picture
Stage | What Happens |
Viral exposure | virus enters body |
Replication | virus copies itself |
Immune response | immune system attacks infected cells |
Chronic inflammation | ongoing damage |
Fibrosis/cirrhosis | architecture changes |
Functional decline | bilirubin, clotting, albumin, portal flow affected |
This is why jaundice may appear late. By the time yellowing is visible, the system may already be under significant stress.
9. Why This Matters in Dentistry
Jaundice and liver disease matter in dental care because the liver affects far more than bilirubin.
Dental Relevance Table
Liver Function | Dental Importance |
Clotting factor synthesis | bleeding risk |
Drug metabolism | medication safety |
Immune function | infection risk |
Bile flow/metabolism | systemic disease clue |
Viral hepatitis status | bloodborne pathogen precautions |
Clinician Thinking
Before care, consider:
Is there known hepatitis B or C?
Is liver disease active or stable?
Is there abnormal bleeding history?
Are medications metabolized by the liver?
Are there signs of ascites, jaundice, fatigue, bruising, or infection risk?
Is medical consultation needed before invasive care?
10. Chairside Explanation
Patient-friendly version
“The yellow color happens when a substance called bilirubin builds up. Bilirubin comes from normal blood cell breakdown, but it has to be processed by the liver and moved out through bile. If too much is made, the liver is injured, or bile flow is blocked, bilirubin can build up and show in the eyes or skin.”
Dental relevance version
“Because the liver also helps with clotting, healing, and medication processing, we may need to adjust treatment or coordinate with your physician before certain dental procedures.”
Clinical Reasoning Framework
When you see jaundice, think through five questions:
Step | Question | Why It Matters |
1 | Is bilirubin overproduced? | pre-hepatic pattern |
2 | Is the liver injured? | hepatic pattern |
3 | Is bile flow blocked? | post-hepatic pattern |
4 | Are there systemic signs? | ascites, itching, infection risk |
5 | Does this change dental care? | bleeding, meds, infection control |
Common Misconceptions
Misconception | Better Understanding |
“Jaundice is a disease.” | It is a sign of an underlying process. |
“Yellow skin always means liver failure.” | It may be pre-hepatic, hepatic, or post-hepatic. |
“If there is no pain, it is not serious.” | Liver disease can be silent for years. |
“Dentistry is unrelated.” | Liver function affects bleeding, medications, and infection risk. |
If You Only Remember One Thing
Jaundice means bilirubin flow is disrupted: too much is produced, the liver cannot process it, or bile cannot carry it out.
ToothOps Insight
Jaundice is not just a color change.
It is a visible map of blood breakdown, liver processing, bile flow, and systemic disease.
Final Takeaway
The best way to understand jaundice is not to memorize yellow skin.
It is to ask:
Where is the bilirubin system failing—production, processing, or flow?
That question turns a symptom into clinical reasoning.
@ToothOps | Fuel Your Smile 😊
Stay tuned for more insights and educational content in our blog.
Disclaimer: Content is for educational purposes only and not a substitute for medical or dental care.
© 2025 ToothOps | All Rights Reserved.



Comments