🧬 Antibody “Upgrades”: How Your Immune System Changes Weapons Without Changing Targets
- ToothOps

- Nov 27, 2025
- 5 min read
Class Switching (B cells) + why it matters for oral & mucosal disease
1️⃣ What Are Antibodies… Really?
Before we talk about class switching, we need to zoom out.
Your immune system makes antibodies — tiny Y-shaped proteins that:
Recognize specific “targets” (antigens) like bacteria, viruses, or even self-tissues
Bind them like a lock and key
Help other immune cells clean up the mess
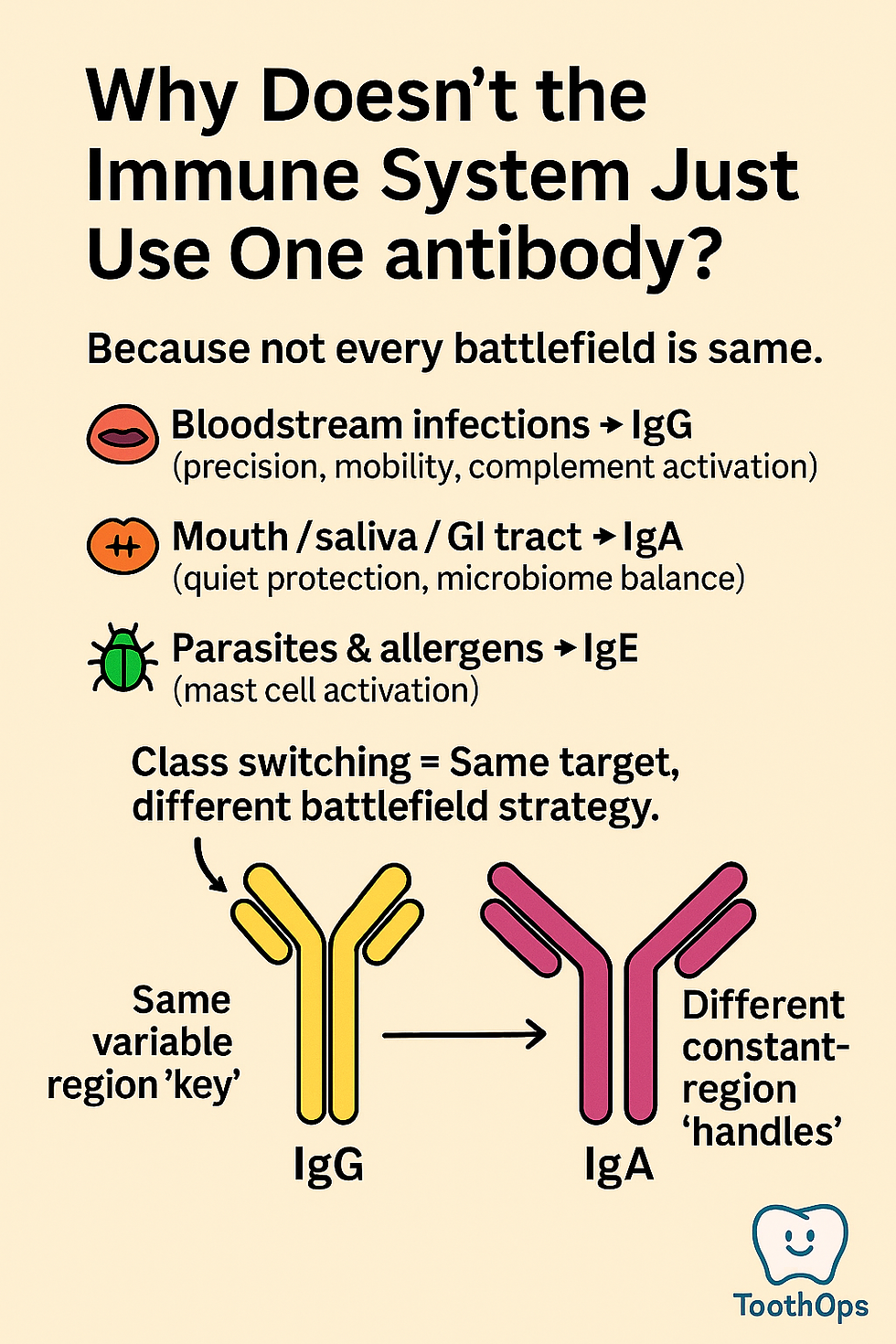
The tip of the Y (the variable region) is the key — it decides what the antibody can recognize.The stem of the Y (the constant region) is the handle — it decides what the antibody can do once it’s bound.
🧠 Analogy:Think of the variable region as your phone’s Face ID (who it recognizes) and the constant region as the app you open (what happens next).Same face → different app → different outcome.

2️⃣ So What Is “Class Switching”?
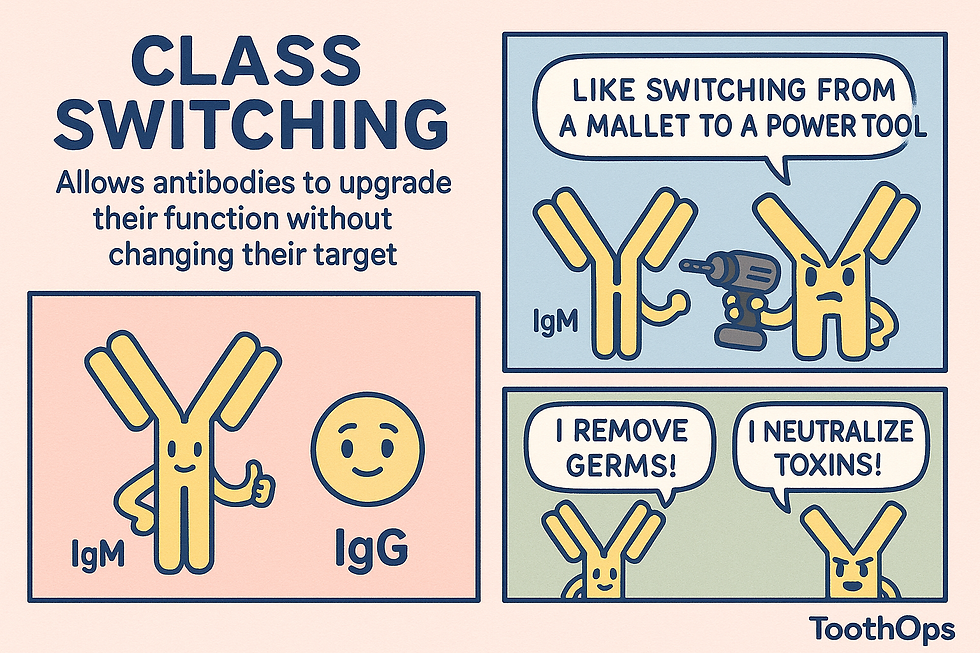
When a B cell first responds to something, it usually makes IgM, a big, early-response antibody. It’s like the rookie responder: fast, loud, and not very precise.
But your body doesn’t stay stuck at “rookie” level.With time and help from other immune cells, that same B cell can switch classes — from IgM to:
IgG – small, powerful, can travel into tissues, activates complement, and opsonizes microbes
IgA – the mucosal protector in saliva, tears, and gut
IgE – the allergy and parasite responder
🚀 Key point:Class Switching = The antibody keeps the same target but upgrades its abilities.
Your B cell doesn’t re-learn the target; it repackages that recognition into a different “antibody body” so it can fight in the right place in the right way.
3️⃣ How Does Class Switching Actually Happen? (Without the Scary Jargon)
Here’s the simplified version of a very complex DNA trick inside B cells:
🧬 Three “Green Lights” Needed:
Antigen binding
Something (bacteria, virus, etc.) binds the B-cell receptor (BCR).
B cell says, “I know this invader.”
T-helper cell permission (CD40–CD40L)
A CD4+ T-helper cell recognizes the same antigen and “talks” to the B cell via CD40L (T cell) and CD40(B cell).
No CD40L = no class switching (this is what happens in hyper-IgM syndrome).
Cytokine “voting system”These are immune signals that tell the B cell which class to switch to:
IL-4 → IgE (and some IgG subclasses)
IFN-γ → IgG
TGF-β + IL-5/IL-6 → IgA
🧠 Analogy:Think of the B cell as a software program getting:
A bug report (antigen)
Approval from the supervisor (T cell)
A feature request (cytokines) saying “we need a mobile app version,” “we need a web app,” etc.
🧬 The DNA Trick (Very Simplified)
Inside the B cell’s nucleus:
There’s a stretch of DNA with the VDJ region (the recognition “key”) followed by multiple constant region genes (Cμ for IgM, Cδ for IgD, Cγ for IgG, Cα for IgA, Cε for IgE).
Special DNA zones called switch (S) regions sit in front of these constant genes.
Then:
The chosen switch region opens up and is transcribed.
An enzyme called AID (activation-induced cytidine deaminase) comes in — this is the molecular scissors.
AID edits cytosines (C) into uracils (U), which flags the DNA for cutting.
DNA repair enzymes create double-stranded breaks at two switch regions.
The DNA loops out the middle chunk and deletes it.
The cell glues the original VDJ (target recognition) to a new constant region (e.g., Cγ for IgG or Cα for IgA).
Result:Same target.New antibody class.Permanent upgrade.

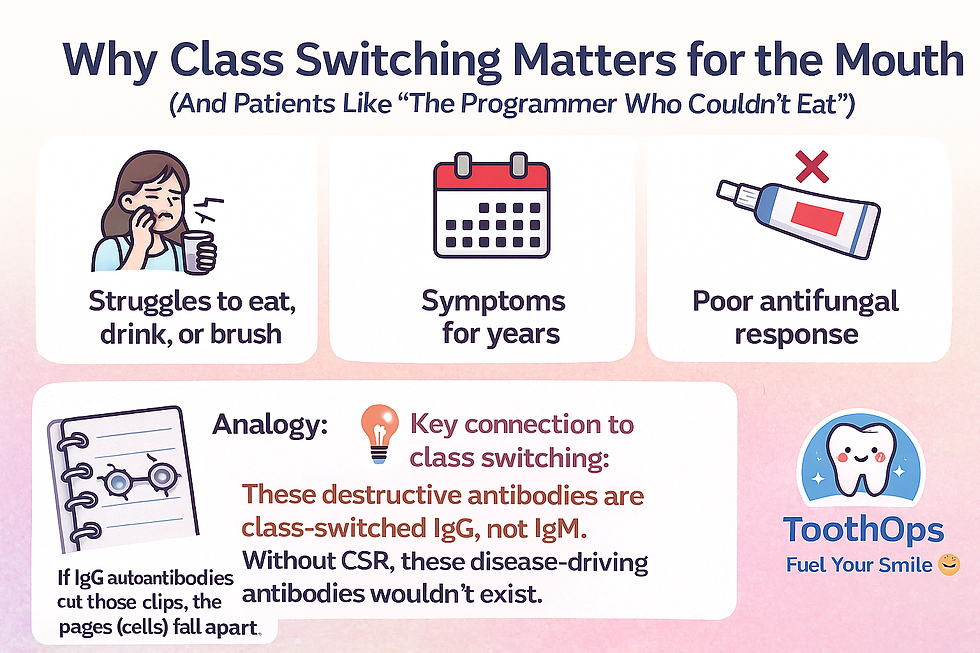
4️⃣ Why Class Switching Matters for the Mouth (And Patients Like “The Programmer Who Couldn’t Eat”)
Imagine a patient who:
Has painful erosions in the mouth, throat, maybe even skin or genital mucosa
Struggles to eat, drink, or brush
Has had symptoms for years
Doesn’t respond well to topical antifungal meds
This pattern screams: “This is not just an infection — this might be autoimmunity.”
In autoimmune blistering diseases (like pemphigus vulgaris):
The immune system makes IgG autoantibodies against desmosomes (the “rivets” holding epithelial cells together).
When those rivets are attacked, cells lose their connections → blisters → erosions → pain.
🧠 Analogy:Think of desmosomes as the metal clips in a spiral notebook.If IgG autoantibodies cut those clips, the pages (cells) fall apart.
💡 Key connection to class switching:These destructive antibodies are class-switched IgG, not IgM.Without CSR, these disease-driving antibodies wouldn’t exist.
5️⃣ Where Does IgA Fit In? (Your Mouth’s Bodyguard)
While IgG is the “sniper” that can be helpful or harmful, IgA is the guardian of your mucosa — especially your mouth.
IgA in saliva:
Coats bacteria so they can’t easily stick to teeth or tissue
Helps maintain a healthy microbiome
Protects against overgrowth of Candida and other pathogens
Reduces inflammation by neutralizing threats quietly
When CSR toward IgA doesn’t work well or IgA is deficient, patients may have:
More frequent oral ulcers
Recurrent candidiasis
Slower wound healing
Chronic irritation and discomfort
For dentists and dental students, this is huge:That “mystery mouth” that never seems to heal might not be “just hygiene” — it might be immune architecture.

6️⃣ Why Lab Tests Care About Class Switching Too
When dermatologists or oral medicine providers order tests like:
Direct immunofluorescence (DIF) – tissue biopsy
Indirect immunofluorescence (IIF) – blood test
They’re looking for IgG and sometimes IgA deposited along the epithelium or circulating in serum.
They are NOT looking for IgM.
Why?Because these diseases are driven by class-switched, affinity-matured antibodies, not the early-phase IgM response.
Class switching makes the difference between:
A short-lived, early immune responsevs.
A chronic, tissue-destructive, autoantibody-driven disease

7️⃣ Clinical Pearls for Dental & Pre-Dental Students
If you’re in clinic (or shadowing) and see:
Long-standing erosive lesions in the mouth
Fragile mucosa that peels or sloughs with gentle manipulation
History of skin involvement or eye irritation
Poor response to antifungals or topical steroids
Your brain should whisper:
“Is there an autoimmune process with class-switched IgG/IgA involved?”
You’re not diagnosing in the chair yet, but you are:
Thinking beyond “canker sores” and “yeast”
Knowing when to refer for biopsy and immunofluorescence
Appreciating that deep immunology → real symptoms → real lives
That’s the level of thinking that turns a provider into a true oral healthcare professional.
8️⃣ Quick Recap
Class Switch Recombination (CSR) = B cell keeps the same antigen target but changes the antibody class (IgM → IgG/IgA/IgE).
It requires antigen, T-helper cell help (CD40–CD40L), and cytokines (e.g., IL-4, IFN-γ, TGF-β).
The enzyme AID cuts DNA at switch regions so the VDJ region can join a new constant region.
IgG = powerful, tissue-penetrating, can drive autoimmune blistering disease.
IgA = mucosal protector in saliva; crucial for oral health and microbial balance.
DIF/IIF tests look for class-switched IgG/IgA, not IgM.
Understanding CSR helps you connect immunology to oral medicine, pathology, and patient care.
@ToothOps | Fuel Your Smile 😊
Stay tuned for more insights and educational content in our blog.
Disclaimer: Content is for educational purposes only and not a substitute for medical or dental care.
© 2025 ToothOps | All Rights Reserved



Comments